
Food is an essential part of life, providing the necessary nutrients and energy to support growth and development. However, for some children, eating can be a source of distress, anxiety, and even fear. This condition is known as Avoidant Restrictive Food Intake Disorder (ARFID), previously known as Selective Eating Disorder or Feeding Disorder of Infancy or Early Childhood. In this blog post, we will explore the various aspects of ARFID, including its symptoms, causes, diagnosis, and treatment.
What is Avoidant Restrictive Food Intake Disorder (ARFID)?
Avoidant Restrictive Food Intake Disorder is a feeding and eating disorder characterized by an ongoing, persistent lack of interest in food, avoidance or restriction of food intake, or avoidance of certain types of food based on their sensory characteristics, such as texture, smell, taste, or appearance. Unlike other eating disorders, such as anorexia nervosa or bulimia nervosa, ARFID does not involve a distorted body image or the desire to lose weight.
Instead, it is primarily a problem with food intake that can result in nutritional deficiencies, poor growth, and weight loss. It can affect children of all ages, from infants to adolescents, and can occur alongside other conditions, such as anxiety disorders, autism spectrum disorder, obsessive-compulsive disorder, or sensory processing disorder. The prevalence of ARFID is estimated to be around 5% of children with feeding and eating difficulties, but the actual number may be higher due to underdiagnosis or misdiagnosis.
What are the Symptoms?
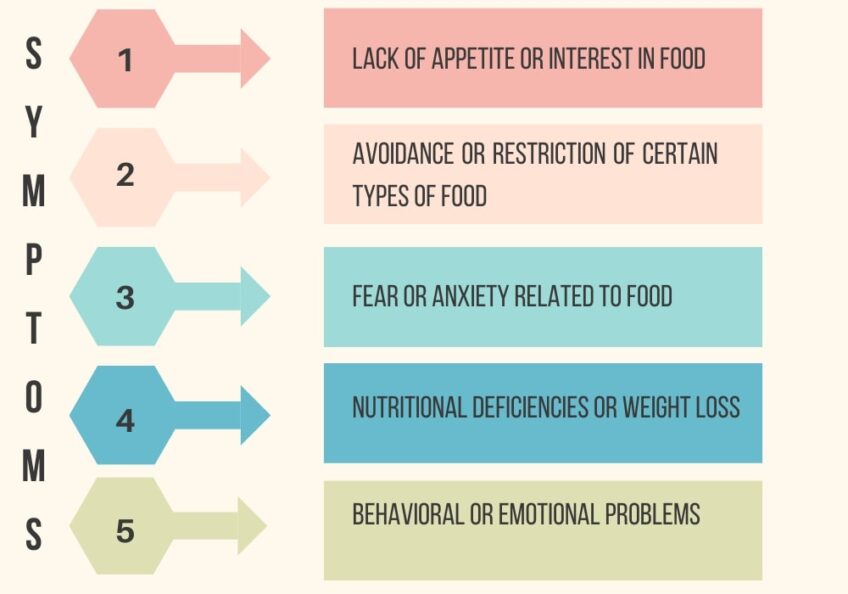
ARFID can manifest in various ways, depending on the severity and type of food avoidance or restriction. Some common symptoms of ARFID include:
Lack of appetite or interest in food: They may have little to no interest in eating or trying new foods. They may be reluctant to approach food or avoid food-related activities, such as mealtime or grocery shopping.
Avoidance or restriction of certain types of food: They may avoid or restrict certain foods based on their sensory characteristics, such as texture, taste, smell, or appearance. They may have a limited range of preferred foods and reject others, leading to a restricted and monotonous diet.
Fear or anxiety related to food: Children with it may experience fear or anxiety related to food, such as fear of choking, vomiting, or allergic reactions. They may also experience anxiety related to social situations involving food, such as eating in public or at school.
Nutritional deficiencies or weight loss: Children with ARFID may have poor growth or weight loss due to inadequate food intake or nutritional deficiencies. They may also have symptoms of malnutrition, such as fatigue, weakness, or gastrointestinal problems.
Behavioral or emotional problems: They may display behavioral or emotional problems related to food, such as tantrums, refusal to eat, or anxiety attacks. They may also have comorbid conditions, such as depression, anxiety, or obsessive-compulsive disorder.
What are the Causes?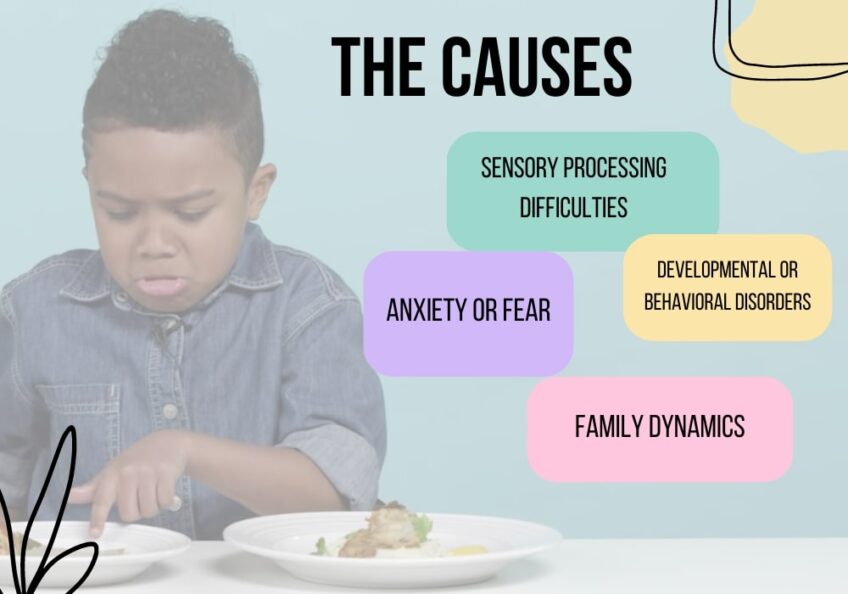
The exact causes of ARFID are not fully understood, but several factors may contribute to its development, such as:
Sensory processing difficulties: Children with ARFID may have sensory processing difficulties, which affect their perception and interpretation of sensory information, such as taste, smell, or texture. They may find certain foods overwhelming, aversive, or intolerable, leading to food avoidance or restriction.
Anxiety or fear: Children with it may have anxiety or fear related to food, such as fear of choking, vomiting, or allergic reactions. This fear may arise from a previous negative experience with food, such as choking or getting sick after eating. It may also be related to other underlying anxiety disorders or trauma.
Developmental or behavioral disorders: Children with it may have underlying developmental or behavioral disorders, such as autism spectrum disorder, attention-deficit/hyperactivity disorder (ADHD), or obsessive-compulsive disorder (OCD). These disorders may affect their eating habits and food preferences.
Family dynamics: Family dynamics may also play a role in the development of ARFID. Children may learn avoidance or restriction of certain foods from their parents or caregivers, who may have their own food preferences or aversions. Family stress or conflict related to food or mealtime may also contribute to the child’s anxiety or avoidance.
How is ARFID Diagnosed?
Diagnosing ARFID involves a comprehensive evaluation by a healthcare professional, such as a pediatrician, psychologist, or dietitian. The evaluation may include a medical history, physical examination, laboratory tests, and psychological assessments. The healthcare professional may also ask the child and their parents or caregivers about their eating habits, food preferences, and behavioral or emotional problems related to food. To be diagnosed with ARFID, the child must meet the following criteria:
- Persistent lack of interest in food, avoidance or restriction of food intake, or avoidance of certain types of food based on sensory characteristics.
- Significant weight loss, nutritional deficiency, dependence on nutritional supplements, or interference with psychosocial functioning.
- Absence of a distorted body image or desire to lose weight, as seen in other eating disorders.
- Symptoms that are not better explained by a medical condition, medication, or other mental disorder.
The role of a multidisciplinary approach in treating ARFID
A multidisciplinary approach is essential because ARFID is a complex disorder that can have physical, psychological, and social consequences for children. The team may include a pediatrician, a psychologist, a dietitian, and an occupational therapist, among others. Each member of the team brings their unique expertise to the treatment plan and collaborates with other professionals to develop an individualized approach to care. The pediatrician plays a key role in the diagnosis and management of ARFID.
They may conduct a physical exam and order laboratory tests to assess the child’s nutritional status and overall health. They may also work with the dietitian to develop a nutrition plan that meets the child’s specific needs and helps them achieve a healthy weight. The psychologist or therapist works with the child to address the emotional and behavioral aspects of ARFID. They may use behavioral therapy, such as cognitive-behavioral therapy or exposure therapy, to help the child overcome their fear and anxiety related to food and expand their range of acceptable foods. They may also work with the parents or caregivers to improve communication and reduce mealtime stress.
The dietitian provides guidance on meal planning, food choices, and gradual exposure to new foods. They may also recommend nutritional supplements or feeding tubes to ensure the child receives adequate nutrients and prevent further weight loss. The occupational therapist works with children who have sensory processing difficulties to improve their ability to tolerate different types of sensory input, including food. They may use sensory integration therapy or other techniques to help the child learn coping strategies and reduce food aversions.
How is ARFID Treated?

The treatment of ARFID depends on the severity and underlying causes of the condition. It may involve a multidisciplinary approach, including medical, nutritional, and psychological interventions. The goals of treatment are to improve the child’s nutritional status, promote healthy eating habits, reduce anxiety and fear related to food, and improve overall psychosocial functioning. Some common treatments for ARFID include:
- Nutritional support: Children with ARFID may require nutritional supplements or feeding tubes to ensure adequate nutrient intake and prevent further weight loss. A registered dietitian can provide guidance on meal planning, food choices, and gradual exposure to new foods.
- Behavioral therapy: Behavioral therapy, such as cognitive-behavioral therapy (CBT) or exposure therapy, can help children overcome their anxiety and fear related to food and expand their range of acceptable foods. The therapy may involve gradual exposure to new foods, positive reinforcement, and coping skills training.
- Medication: In some cases, medication may be prescribed to treat underlying anxiety or depression that may be contributing to ARFID.
- Family therapy: Family therapy can help improve communication and relationships related to food and mealtime. It can also help parents or caregivers develop strategies to support their child’s eating habits and reduce mealtime stress or conflict.
- Occupational therapy: Occupational therapy can help children with sensory processing difficulties learn coping strategies and improve their ability to tolerate different types of sensory input, including food.
Medications for children with ARFID
Anxiety and depression can often co-occur with ARFID and can make it difficult for children to eat and try new foods. In such cases, medication can be an important part of the treatment plan. Selective serotonin reuptake inhibitors (SSRIs) are commonly prescribed to treat anxiety and depression in children with ARFID. SSRIs work by increasing the amount of serotonin in the brain, which can improve mood and reduce anxiety. Common SSRIs prescribed for children with ARFID include fluoxetine (Prozac), sertraline (Zoloft), and escitalopram (Lexapro).
Other medications that may be used to treat anxiety and depression in children with ARFID include tricyclic antidepressants (TCAs), benzodiazepines, and beta-blockers. However, these medications are typically used less frequently in children due to their potential side effects and safety concerns. It is important to note that medication should only be prescribed by a qualified healthcare professional, such as a pediatrician or psychiatrist. The decision to prescribe medication will depend on the severity of the child’s symptoms, the potential benefits and risks of the medication, and the child’s overall health and medical history.
FAQs
What is occupational therapy, and how is it used to treat ARFID?
Occupational therapy can help children with sensory processing difficulties learn coping strategies and improve their ability to tolerate different types of sensory input, including food.
Can ARFID be cured?
There is no cure for ARFID, but with appropriate treatment, children with it can overcome their fears and aversions related to food and develop healthy eating habits for a lifetime.
How can parents or caregivers support a child with ARFID at home?
Parents or caregivers can support a child with it by offering a variety of foods, creating a calm and positive environment during mealtimes, and seeking professional help if they suspect that their child may have ARFID.
Why is early intervention important in treating ARFID?
Early intervention is important in treating it because it can improve outcomes and prevent further complications. The earlier ARFID is diagnosed and treated, the better the chances for a successful recovery. Early intervention can also prevent the development of more severe eating disorders and associated mental health problems. Therefore, it is essential for parents or caregivers to seek professional help if they suspect that their child may have it.
Can nutritional supplements or feeding tubes be used to treat ARFID?
Yes, nutritional supplements or feeding tubes may be used to ensure adequate nutrient intake and prevent further weight loss in children with ARFID.
Conclusion
Avoidant Restrictive Food Intake Disorder is a feeding and eating disorder that affects children of all ages. It is characterized by a persistent lack of interest in food, avoidance or restriction of food intake, or avoidance of certain types of food based on sensory characteristics. It can result in nutritional deficiencies, poor growth, and weight loss, and can have a significant impact on the child’s psychosocial functioning. It is important to seek professional help if you suspect that your child may have ARFID, as early intervention can improve outcomes and prevent further complications.